
You searched for:"Alexandre Biasi Cavalcanti"
We found (31) results for your search.-
Clinical Report
Prospective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
- ,
- Israel Silva Maia
 ,
, - Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini , [ … ],
- Fernando Godinho Zampieri
Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views77ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee moreViews77

Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views77ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee more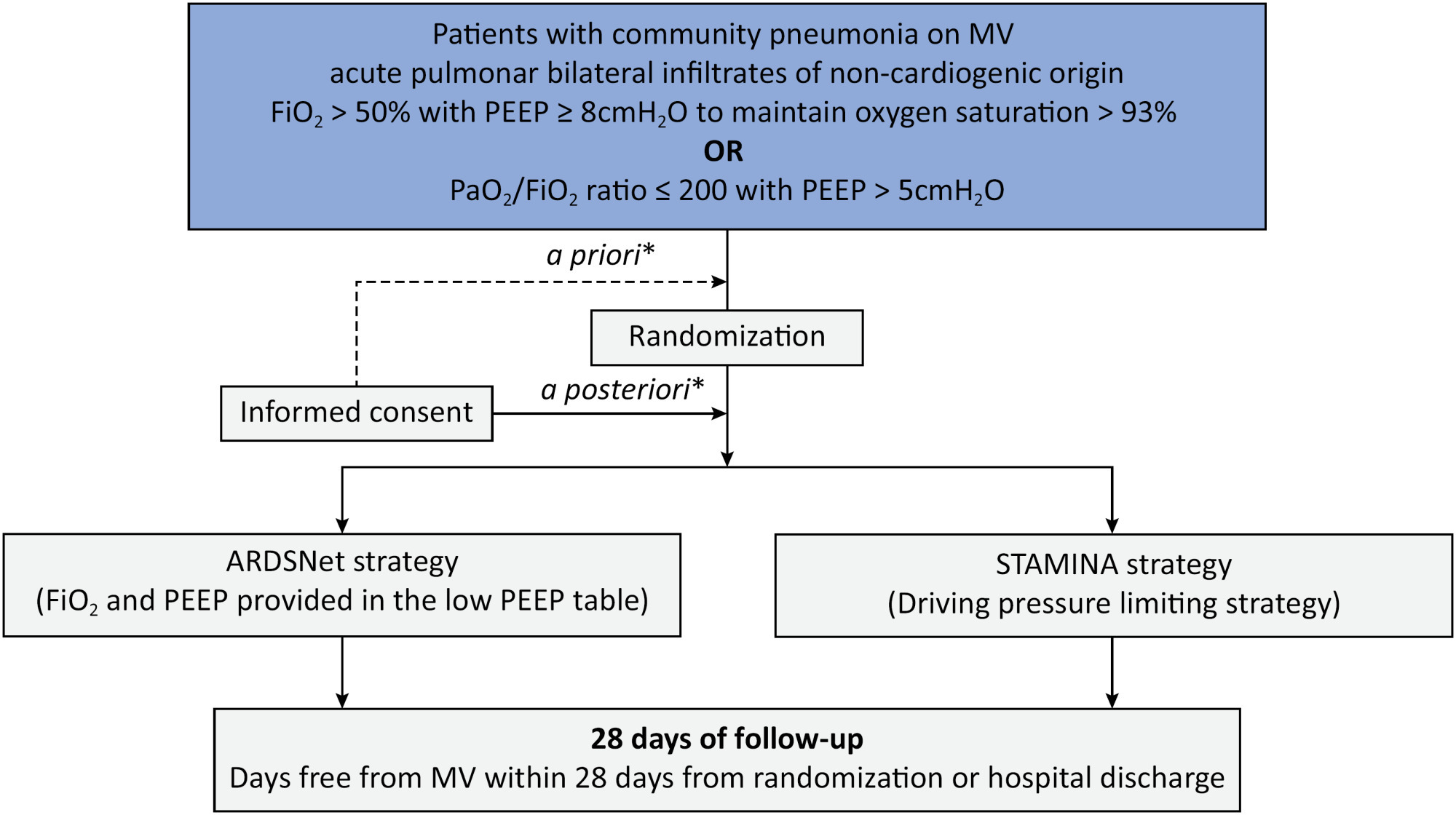
-
Editorial
Challenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See moreViews25Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See more -
Special Article
Intensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi , [ … ],
- Simon Finfer
Abstract
Special ArticleIntensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
Crit Care Sci. 2023;35(4):345-354
DOI 10.5935/2965-2774.20230162-pt
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi ,
- Federico Bilotta ,
- Julien Bohé ,
- Frank Martin Brunkhorst ,
- Alexandre Biasi Cavalcanti ,
- Deborah Cook,
- Christoph Engel,
- Deborah Green-LaRoche ,
- Wei He,
- William Henderson,
- Cornelia Hoedemaekers ,
- Gaetano Iapichino ,
- Pierre Kalfon ,
- Gisela de La Rosa ,
- Iain MacKenzie,
- Christian Mélot ,
- Imogen Mitchell ,
- Tuomas Oksanen,
- Federico Polli ,
- Jean-Charles Preiser ,
- Francisco Garcia Soriano ,
- Ling-Cong Wang,
- Jiaxiang Yuan,
- Anthony Delaney ,
- Gian Luca Di Tanna ,
- Simon Finfer
Views19ABSTRACT
Objective:
The optimal target for blood glucose concentration in critically ill patients is unclear. We will perform a systematic review and meta-analysis with aggregated and individual patient data from randomized controlled trials, comparing intensive glucose control with liberal glucose control in critically ill adults.
Data sources:
MEDLINE®, Embase, the Cochrane Central Register of Clinical Trials, and clinical trials registries (World Health Organization, clinical trials.gov). The authors of eligible trials will be invited to provide individual patient data. Published trial-level data from eligible trials that are not at high risk of bias will be included in an aggregated data meta-analysis if individual patient data are not available.
Methods:
Inclusion criteria: randomized controlled trials that recruited adult patients, targeting a blood glucose of ≤ 120mg/dL (≤ 6.6mmol/L) compared to a higher blood glucose concentration target using intravenous insulin in both groups. Excluded studies: those with an upper limit blood glucose target in the intervention group of > 120mg/dL (> 6.6mmol/L), or where intensive glucose control was only performed in the intraoperative period, and those where loss to follow-up exceeded 10% by hospital discharge.
Primary endpoint:
In-hospital mortality during index hospital admission. Secondary endpoints: mortality and survival at other timepoints, duration of invasive mechanical ventilation, vasoactive agents, and renal replacement therapy. A random effect Bayesian meta-analysis and hierarchical Bayesian models for individual patient data will be used.
Discussion:
This systematic review with aggregate and individual patient data will address the clinical question, ‘what is the best blood glucose target for critically ill patients overall?’
Keywords:Blood glucoseCritical illnessGlycemic controlinsulinIntraoperative periodMortalityPatient dischargeRegistriesSee moreViews19Abstract
Special ArticleIntensive glucose control in critically ill adults: a protocol for a systematic review and individual patient data meta-analysis
Crit Care Sci. 2023;35(4):345-354
DOI 10.5935/2965-2774.20230162-pt
- Derick Adigbli ,
- Li Yang,
- Naomi Hammond ,
- Djillali Annane,
- Yaseen Arabi ,
- Federico Bilotta ,
- Julien Bohé ,
- Frank Martin Brunkhorst ,
- Alexandre Biasi Cavalcanti ,
- Deborah Cook,
- Christoph Engel,
- Deborah Green-LaRoche ,
- Wei He,
- William Henderson,
- Cornelia Hoedemaekers ,
- Gaetano Iapichino ,
- Pierre Kalfon ,
- Gisela de La Rosa ,
- Iain MacKenzie,
- Christian Mélot ,
- Imogen Mitchell ,
- Tuomas Oksanen,
- Federico Polli ,
- Jean-Charles Preiser ,
- Francisco Garcia Soriano ,
- Ling-Cong Wang,
- Jiaxiang Yuan,
- Anthony Delaney ,
- Gian Luca Di Tanna ,
- Simon Finfer
Views19ABSTRACT
Objective:
The optimal target for blood glucose concentration in critically ill patients is unclear. We will perform a systematic review and meta-analysis with aggregated and individual patient data from randomized controlled trials, comparing intensive glucose control with liberal glucose control in critically ill adults.
Data sources:
MEDLINE®, Embase, the Cochrane Central Register of Clinical Trials, and clinical trials registries (World Health Organization, clinical trials.gov). The authors of eligible trials will be invited to provide individual patient data. Published trial-level data from eligible trials that are not at high risk of bias will be included in an aggregated data meta-analysis if individual patient data are not available.
Methods:
Inclusion criteria: randomized controlled trials that recruited adult patients, targeting a blood glucose of ≤ 120mg/dL (≤ 6.6mmol/L) compared to a higher blood glucose concentration target using intravenous insulin in both groups. Excluded studies: those with an upper limit blood glucose target in the intervention group of > 120mg/dL (> 6.6mmol/L), or where intensive glucose control was only performed in the intraoperative period, and those where loss to follow-up exceeded 10% by hospital discharge.
Primary endpoint:
In-hospital mortality during index hospital admission. Secondary endpoints: mortality and survival at other timepoints, duration of invasive mechanical ventilation, vasoactive agents, and renal replacement therapy. A random effect Bayesian meta-analysis and hierarchical Bayesian models for individual patient data will be used.
Discussion:
This systematic review with aggregate and individual patient data will address the clinical question, ‘what is the best blood glucose target for critically ill patients overall?’
Keywords:Blood glucoseCritical illnessGlycemic controlinsulinIntraoperative periodMortalityPatient dischargeRegistriesSee more - Derick Adigbli
-
Original Article
Effects of balanced solution on short-term outcomes in traumatic brain injury patients: a secondary analysis of the BaSICS randomized trial
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende Freitas ,
- Viviane Cordeiro Veiga , [ … ],
Abstract
Original ArticleEffects of balanced solution on short-term outcomes in traumatic brain injury patients: a secondary analysis of the BaSICS randomized trial
Rev Bras Ter Intensiva. 2022;34(4):410-417
DOI 10.5935/0103-507X.20220261-en
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende Freitas ,
- Viviane Cordeiro Veiga ,
- Rodrigo Cruvinel Figueiredo,
- Ary Serpa-Neto ,
- Airton Leonardo de Oliveira Manoel ,
- Tamiris Abait Miranda,
- Thiago Domingos Corrêa ,
- Luciano César Pontes de Azevedo ,
- Nilton Brandão da Silva ,
- Flavia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
Views2ABSTRACT
Objective:
To describe the effects of balanced solution use on the short-term outcomes of patients with traumatic brain injury enrolled in BaSICS trial.
Methods:
Patients were randomized to receive either 0.9% saline or balanced solution during their intensive care unit stay. The primary endpoint was 90-day mortality, and the secondary outcomes were days alive and free of intensive care unit stay at 28 days. The primary endpoint was assessed using Bayesian logistic regression. The secondary endpoint was assessed using a Bayesian zero-inflated beta binomial regression.
Results:
We included 483 patients (236 in the 0.9% saline arm and 247 in the balanced solution arm). A total of 338 patients (70%) with a Glasgow coma scale score ≤ 12 were enrolled. The overall probability that balanced solutions were associated with higher 90-day mortality was 0.98 (OR 1.48; 95%CrI 1.04 – 2.09); this mortality increment was particularly noticeable in patients with a Glasgow coma scale score below 6 at enrollment (probability of harm of 0.99). Balanced solutions were associated with -1.64 days alive and free of intensive care unit at 28 days (95%CrI -3.32 – 0.00) with a probability of harm of 0.97.
Conclusion:
There was a high probability that balanced solutions were associated with high 90-day mortality and fewer days alive and free of intensive care units at 28 days.
Keywords:Balanced solutionsBrain injuriesCritical careHospital mortalityMortalitySaline solutiontraumaticSee moreViews2Abstract
Original ArticleEffects of balanced solution on short-term outcomes in traumatic brain injury patients: a secondary analysis of the BaSICS randomized trial
Rev Bras Ter Intensiva. 2022;34(4):410-417
DOI 10.5935/0103-507X.20220261-en
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende Freitas ,
- Viviane Cordeiro Veiga ,
- Rodrigo Cruvinel Figueiredo,
- Ary Serpa-Neto ,
- Airton Leonardo de Oliveira Manoel ,
- Tamiris Abait Miranda,
- Thiago Domingos Corrêa ,
- Luciano César Pontes de Azevedo ,
- Nilton Brandão da Silva ,
- Flavia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
Views2ABSTRACT
Objective:
To describe the effects of balanced solution use on the short-term outcomes of patients with traumatic brain injury enrolled in BaSICS trial.
Methods:
Patients were randomized to receive either 0.9% saline or balanced solution during their intensive care unit stay. The primary endpoint was 90-day mortality, and the secondary outcomes were days alive and free of intensive care unit stay at 28 days. The primary endpoint was assessed using Bayesian logistic regression. The secondary endpoint was assessed using a Bayesian zero-inflated beta binomial regression.
Results:
We included 483 patients (236 in the 0.9% saline arm and 247 in the balanced solution arm). A total of 338 patients (70%) with a Glasgow coma scale score ≤ 12 were enrolled. The overall probability that balanced solutions were associated with higher 90-day mortality was 0.98 (OR 1.48; 95%CrI 1.04 – 2.09); this mortality increment was particularly noticeable in patients with a Glasgow coma scale score below 6 at enrollment (probability of harm of 0.99). Balanced solutions were associated with -1.64 days alive and free of intensive care unit at 28 days (95%CrI -3.32 – 0.00) with a probability of harm of 0.97.
Conclusion:
There was a high probability that balanced solutions were associated with high 90-day mortality and fewer days alive and free of intensive care units at 28 days.
Keywords:Balanced solutionsBrain injuriesCritical careHospital mortalityMortalitySaline solutiontraumaticSee more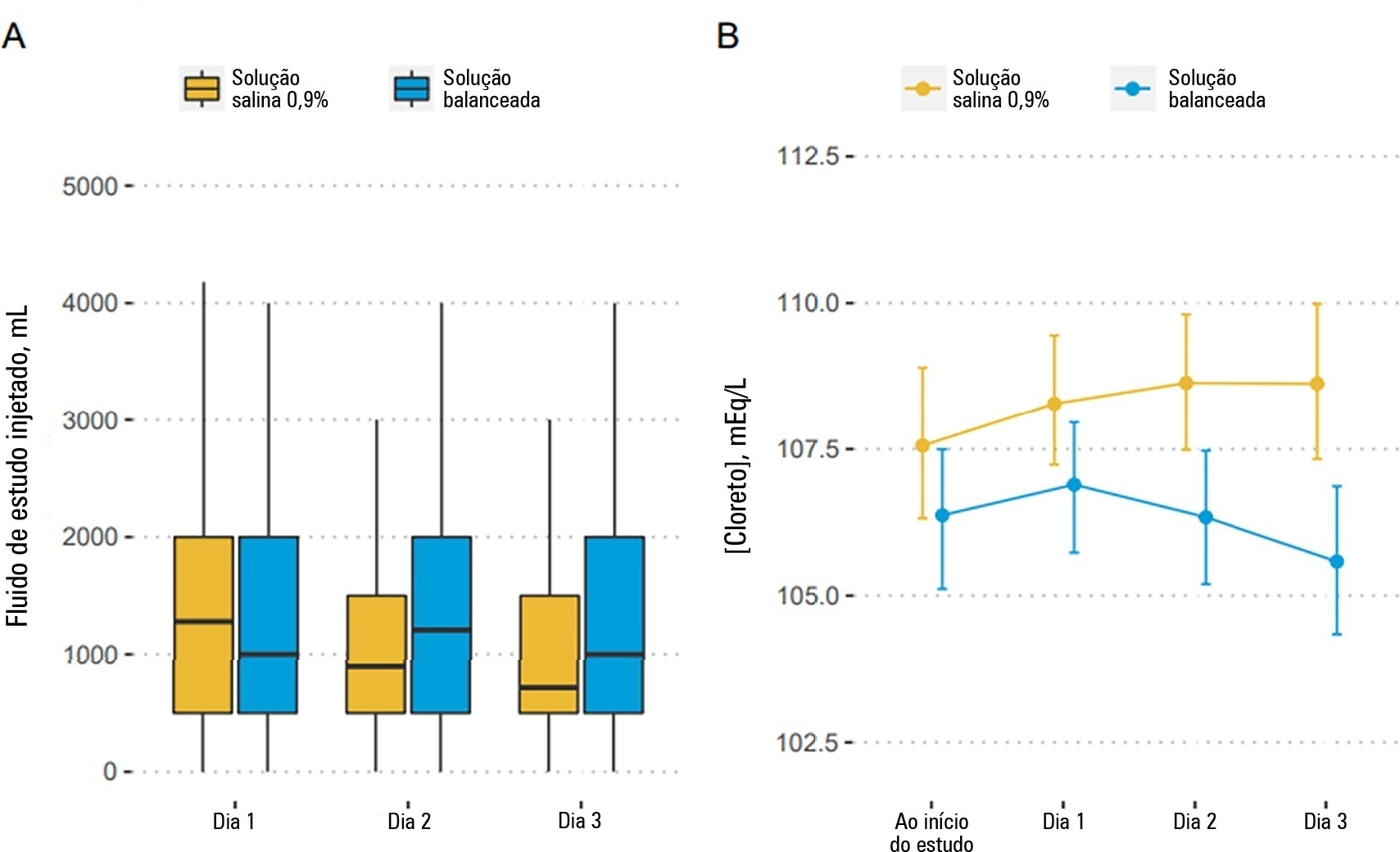
- Fernando Godinho Zampieri
-
Original Article
IMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee moreViews2Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee more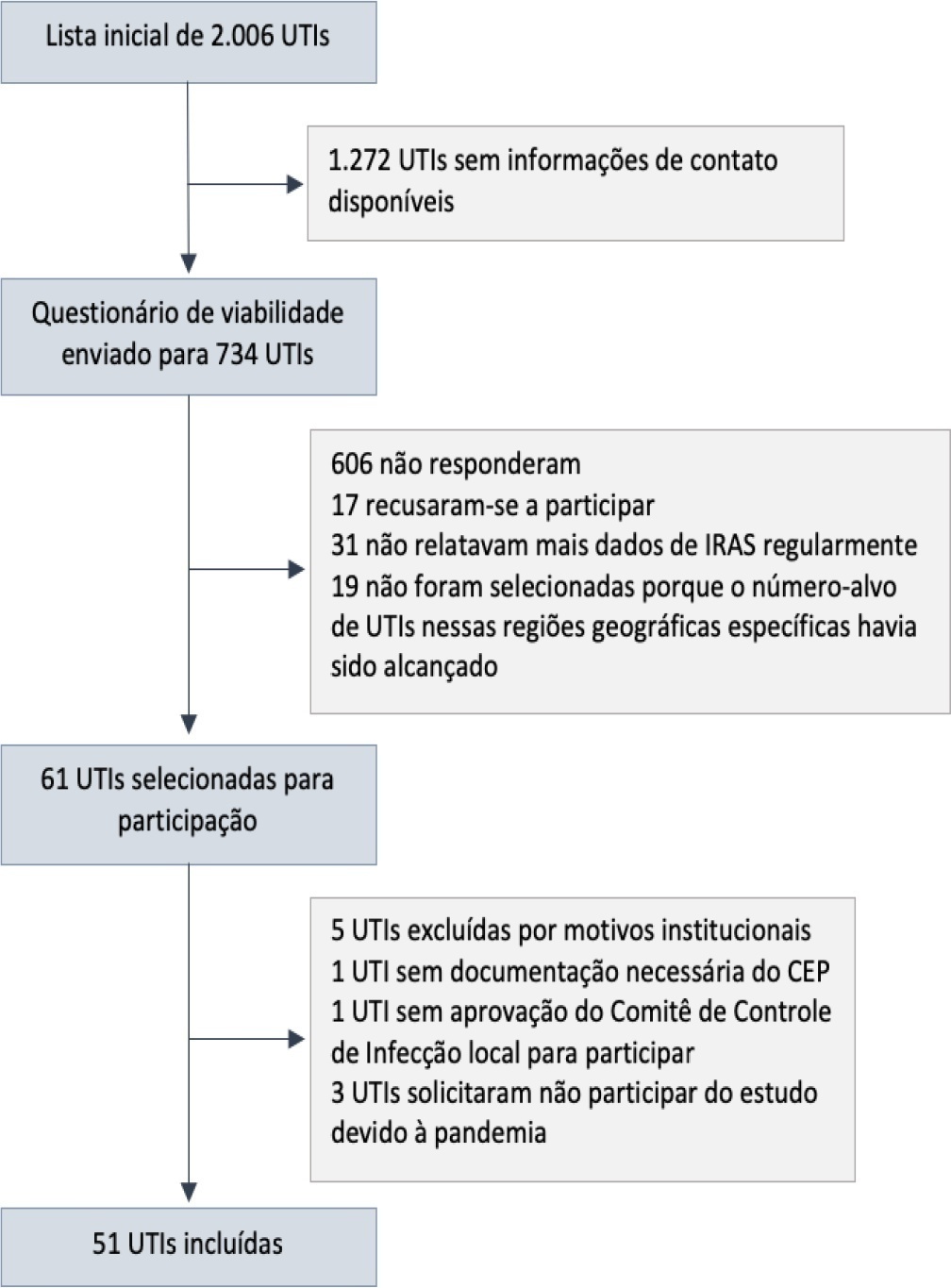
- Bruno M Tomazini
-
Special Article
Automated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak , [ … ],
- Aline Marcadenti
Abstract
Special ArticleAutomated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
Rev Bras Ter Intensiva. 2022;34(3):319-326
DOI 10.5935/0103-507X.20220101-en
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak ,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel ,
- Samira Martins Tokunaga ,
- Karina Leal Negrelli ,
- Gabriela Souza Murizine ,
- Fernando Medrado Júnior ,
- Rita de Cassia Pires Coli ,
- Alexandre Biasi Cavalcanti ,
- Aline Marcadenti
Views2ABSTRACT
Objective:
To evaluate the effectiveness of the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ solution in activating the rapid response team in a timely manner compared to manual activation.
Methods:
The Hillrom study is a single-center, open-label, superiority, cluster-randomized, parallel-group (1:1 allocation ratio) clinical trial that will be conducted in a tertiary hospital. Two sets of three wards with 28 beds will be included (one as the intervention cluster and the other as the control). The wards will be randomly assigned to use the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution (intervention cluster) or to maintain the usual routine (control cluster) regarding rapid response team activation. The primary outcome will be the absolute number of episodes of rapid response team triggering in an appropriate time; as secondary outcomes, clinical features (mortality, cardiac arrest, need for intensive care unit admission and duration of hospitalization) will be assessed according to clusters in an exploratory way. A sample size of 216 rapid response team activations was estimated to identify a possible difference between the groups. The protocol has been approved by the institutional Research Ethics Committee.
Expected results:
The Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution is expected to be more effective in triggering the nurse call system to activate the rapid response team in a timely and adequate manner compared to manual triggering (usual practice).
ClinicalTrials.gov:
NCT04648579
Keywords:computerizedHealth information interoperabilityHospital rapid response teamMedical records systemsNursing stationsVital signsSee moreViews2Abstract
Special ArticleAutomated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
Rev Bras Ter Intensiva. 2022;34(3):319-326
DOI 10.5935/0103-507X.20220101-en
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak ,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel ,
- Samira Martins Tokunaga ,
- Karina Leal Negrelli ,
- Gabriela Souza Murizine ,
- Fernando Medrado Júnior ,
- Rita de Cassia Pires Coli ,
- Alexandre Biasi Cavalcanti ,
- Aline Marcadenti
Views2ABSTRACT
Objective:
To evaluate the effectiveness of the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ solution in activating the rapid response team in a timely manner compared to manual activation.
Methods:
The Hillrom study is a single-center, open-label, superiority, cluster-randomized, parallel-group (1:1 allocation ratio) clinical trial that will be conducted in a tertiary hospital. Two sets of three wards with 28 beds will be included (one as the intervention cluster and the other as the control). The wards will be randomly assigned to use the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution (intervention cluster) or to maintain the usual routine (control cluster) regarding rapid response team activation. The primary outcome will be the absolute number of episodes of rapid response team triggering in an appropriate time; as secondary outcomes, clinical features (mortality, cardiac arrest, need for intensive care unit admission and duration of hospitalization) will be assessed according to clusters in an exploratory way. A sample size of 216 rapid response team activations was estimated to identify a possible difference between the groups. The protocol has been approved by the institutional Research Ethics Committee.
Expected results:
The Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution is expected to be more effective in triggering the nurse call system to activate the rapid response team in a timely and adequate manner compared to manual triggering (usual practice).
ClinicalTrials.gov:
NCT04648579
Keywords:computerizedHealth information interoperabilityHospital rapid response teamMedical records systemsNursing stationsVital signsSee more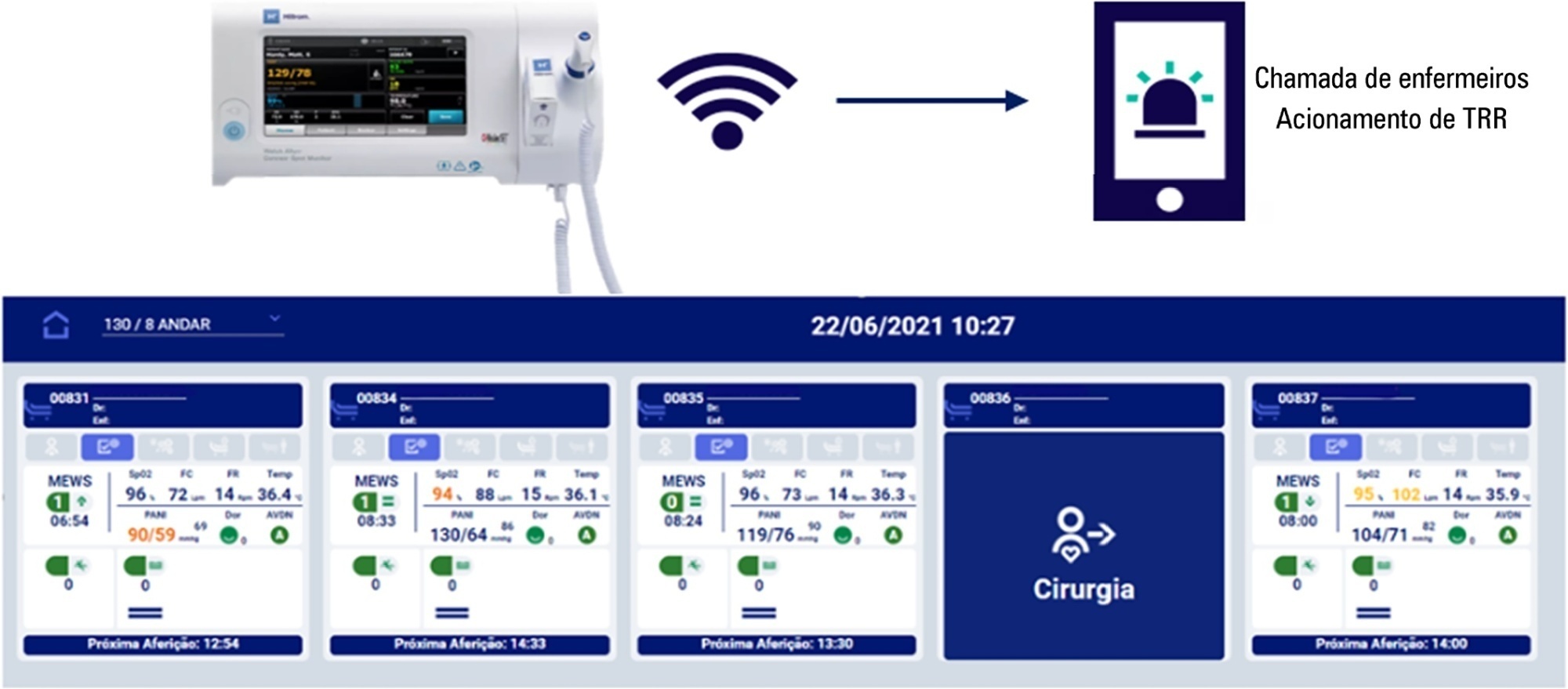
- José Cesar Ribeiro
-
Original Article
Clinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho , [ … ],
- Luciano César Pontes de Azevedo
Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee moreViews3Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee more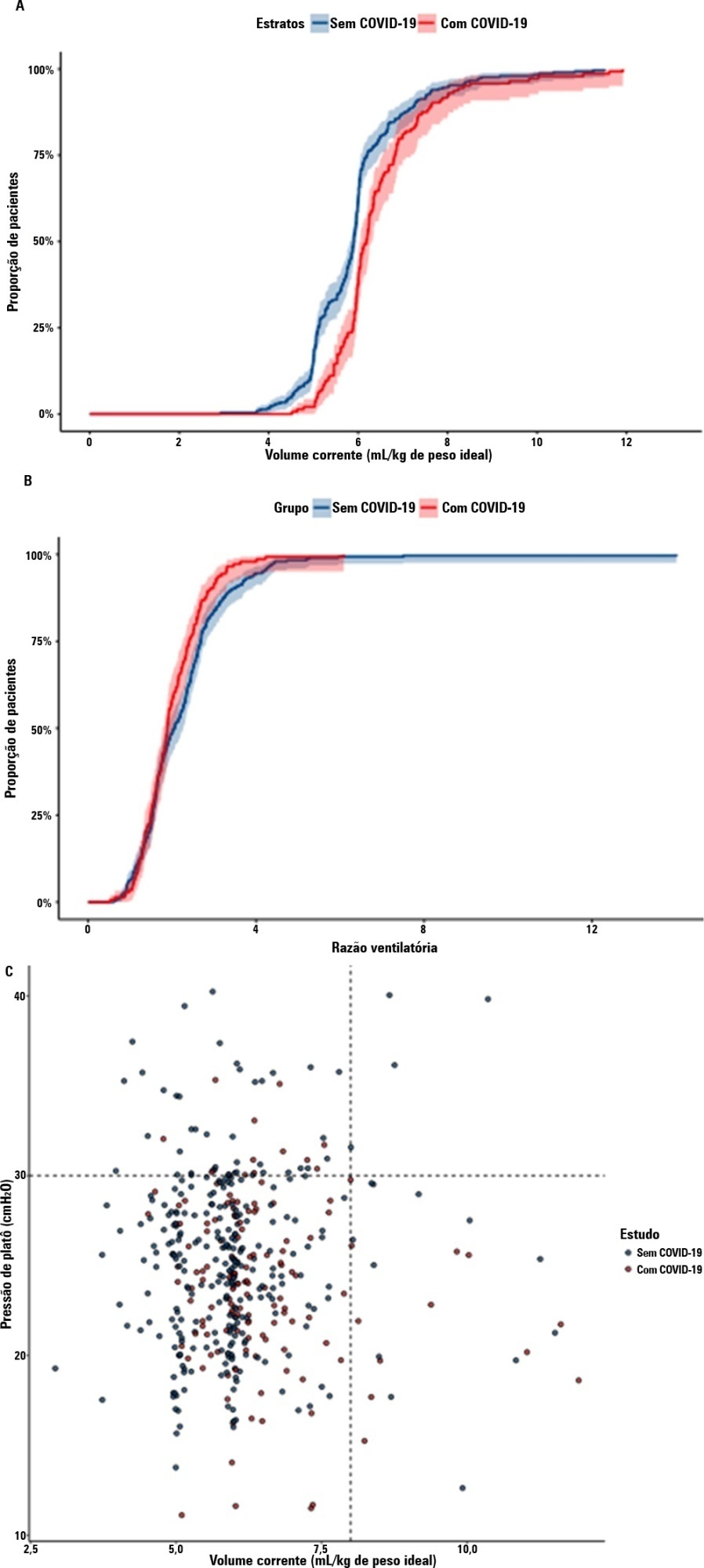
- Bruno Martins Tomazini
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis